LABORATORY TESTING FOR INFLAMMATION
Acute phase reactants are proteins whose concentration changes by >25% in the presence of inflammation (acute or chronic), Positive acute phase proteins increase in inflammation and include CRP, fibrinogen, serum amyloid A, alpha-1 antitrypsin, haptoglobins and ferritin. Negative acute phase proteins decrease in inflammation and include albumin, transferrin and transthyretin.
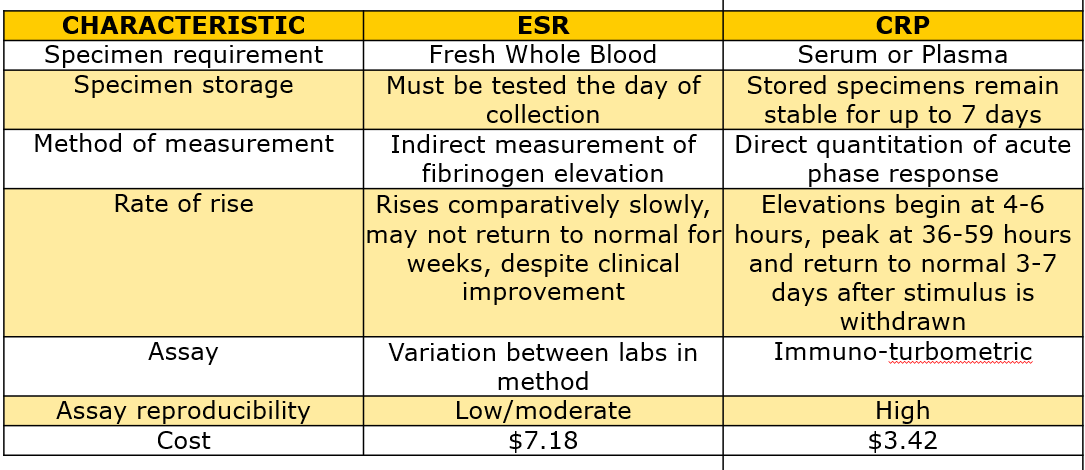
CRP is part of the innate immune system and levels rise with 4-6 hours of an inflammatory stimulus, returning to normal 3.7 days after the stimulus is withdrawn. It is a direct measure of the acute phase response.
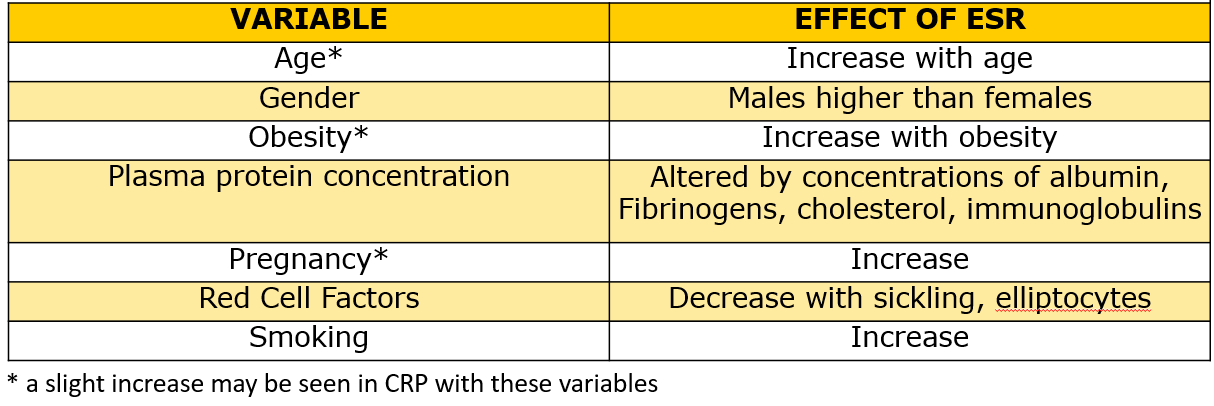
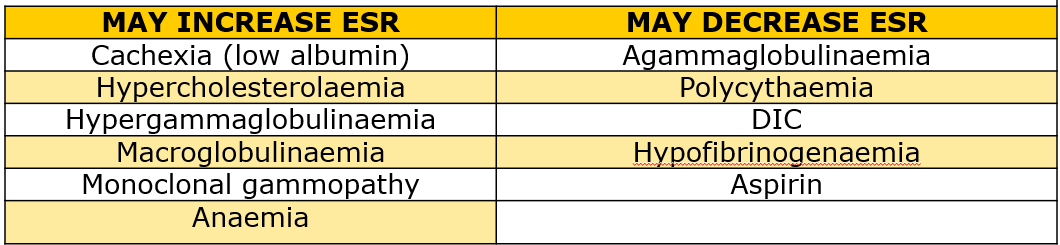
ESR is the rate at which erythrocytes settle when placed in a vertical tube. This depends primarily on the concentration of fibrinogen, which is an acute phase reactant. The ESR is an indirect measure of the acute phase response. As listed below, a number of other factors, some physiological, same disease-related and some related to the test system can influence the rate at which red cells settle when placed in a vertical tube. Furthermore, the rate of rise following a stimulus is comparatively slow and the ESR may not return to normal for weeks, despite clinical improvement.
Laboratory Testing Factors which alter the result of the ESR
A) Test Method
There are a number of methods available to determine the ESR. The two test systems used by Middlemore Hospital use the standard Westergren method in accordance with the Clinical and Laboratory Standards Institute (CLSI), they are:
· An automated analyser exclusively employed for analysis of the erythrocyte sedimentation rate with a measuring range of 1 140mm/hour. This method is a corrected method that takes 30 minutes.
· A manual method using Microvette 200 ESR method which only requires 200µL of blood, this method takes a full one hour.
There can be variation between the results obtained by these methods however routine quality control measures are carried out to compare the methods and ensure there is an acceptable variation between results. The automated method is the preferred method which requires a minimum of 1.3mL of EDTA blood.
B) Precision
There are little reliable data because of the large specimen volumes required to run duplicate testing.
C) Quality Control Material
Laboratory tests undergo regular quality control using both internal and external quality assurance material which requires stabilized controls. These are ordered for daily ESR QC and in addition, routine external quality controls (RCPA) are run twice a year.
Performance of CRP and ESR for specific applications
1) Rheumatoid Arthritis
The ESR has been more widely used for the purpose of disease activity monitoring in RA. Elevations of both CRP and ESR are associated with radiographic progression.
2) Polymyalgia rheumatica and giant cell arteritis
Whilst these diseases are frequently accompanied by an increase in ESR, 7-20% of patients may have normal ESR. What constitutes a "normal" ESR level in the elderly can also hamper interpretation of this result. CRP and ESR are considered to be of approximately equal value in assessing disease activity.
3) Systemic Lupus Erythematosis
Many patients with active SLE do not have elevated CRP concentrations.
4) Chronic lnfections
The slow rate of fall of the ESR makes the CRP more useful in assessing response.
5) Kawasaki disease
Both ESR and CRP are increased.
6) Rheumatic fever
Both ESR and CRP may be increased. CRP can rise nonspecifically with heart failure and, therefore, in some cases, an ESR may provide additional information.
7) Hodgkins Lymphoma/ Non Hodgkins
An ESR of greater than 70 may represent a poor prognosis in this disease. As with both CRP and ESR any infection in the patient will cause a rise in both these tests.
8) Temporal Arteritis
In temporal arteritis both the CRP and the ESR are usually elevated. However recent references indicate that the CRP has a greater sensitivity at 97.5% compared to 76-86% for the ESR. If both tests are used there is a sensitivity of 99.2%. The reference paper recommends that only the CRP be done and states that any patient with a strong history should have a temporal biopsy or empirical treatment irrespective of the lab results.
9) Protein Dyscrasias
10) Autoimmune disease
{kind=link}
{kind=link}
{kind=link}
{kind=link}